



Progressive Pulmonary Fibrosis Management in Real-World Setting – The PROFIBRO Survey
Authors & Institutions
M. Mehta¹, Sujeet R², Y. Sivagnaname³, V.K. Chennamchetty⁴, S. Singh⁵, M. Shah⁶, S. Krishnan⁷, K. Krishnamurthy⁸, D. Muthreja⁹, R. Jalan¹⁰, S. Tale¹¹, M. Lopez¹, S. Mohanasundaram¹, J. Gogtay¹
¹Cipla Ltd, India; other co-authors from major hospitals across India.
Introduction
- Progressive pulmonary fibrosis (PPF) constitutes 13–40% of fibrotic interstitial lung diseases (F-ILD).
- Limited Indian data available on real-world PPF management.
Objective
- To understand management patterns of PPF in real-world clinical settings.
Methodology
- Clinicians attending CME programs (Jan–Dec 2024) on respiratory diseases completed a survey questionnaire.
- 117 clinicians from 16 Indian states participated (87% pulmonologists).
- Results expressed as percentages based on responses.
Results
PPF Diagnosis
- 50% based diagnosis on clinical judgment with radiologic and lung function findings.
- 42%, 6%, and 2% followed 2022 ATS/ERS/ALAT/JRS, INBUILD, and RELIEF criteria respectively.
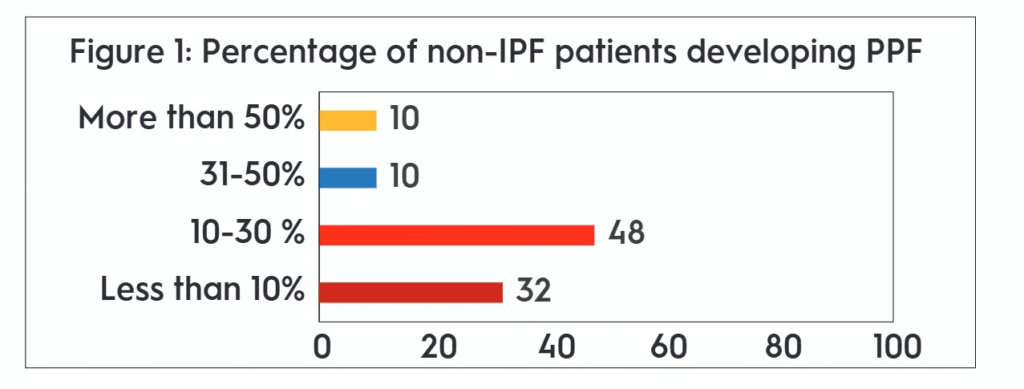
Prevalence of PPF among F-ILD patients
- 48% clinicians: 10–30% of their F-ILD patients develop PPF.
- 32%: <10% (Figure 1).
Diagnosis and Monitoring
- 39% labelled F-ILD as PPF regardless of fibrosis duration.
- 27% labelled after 12 months, 21% after 6 months.
- Commonly associated ILDs:
- F-HP (85%)
- RA-ILD (72%)
- Preferred monitoring tools:
- FVC (89%), HRCT (88%), 6MWD (84%)
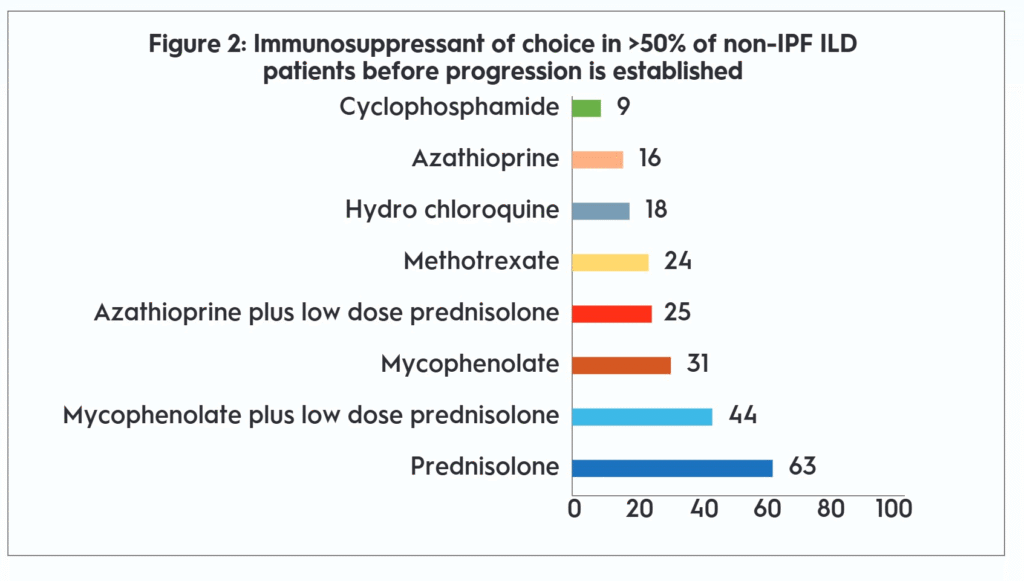
Treatment Practices
Before Progression
- 63% used prednisolone in >50% of non-IPF ILD patients before progression.
- 44% preferred combination of mycophenolate + low-dose prednisolone (Figure 2).
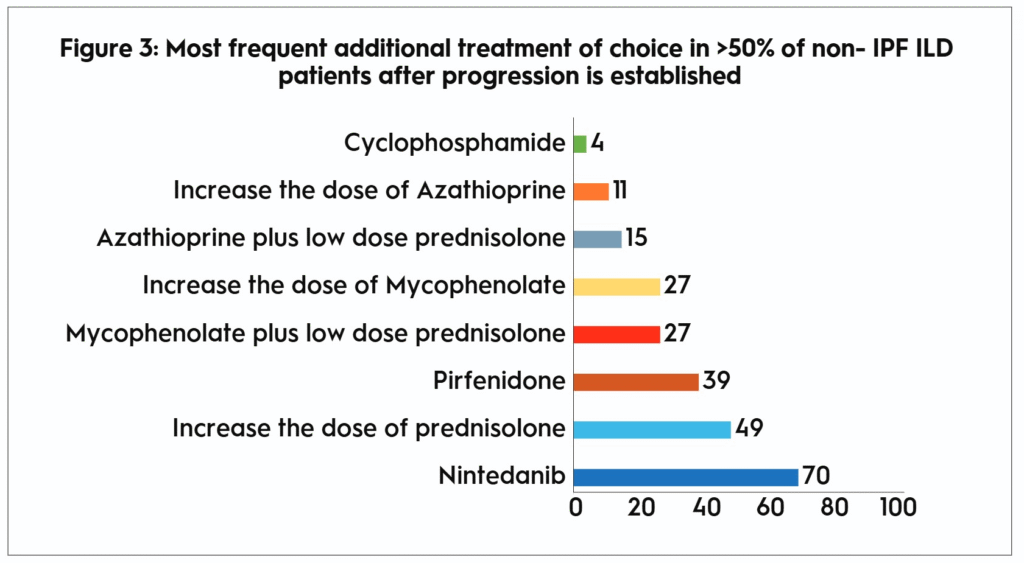
After Progression
- Most frequent additional treatments (>50% of cases) (Figure 3):
- Nintedanib (70%)
- Increase dose of prednisolone (49%)
- Pirfenidone (39%)
- Mycophenolate ± prednisolone (27%)
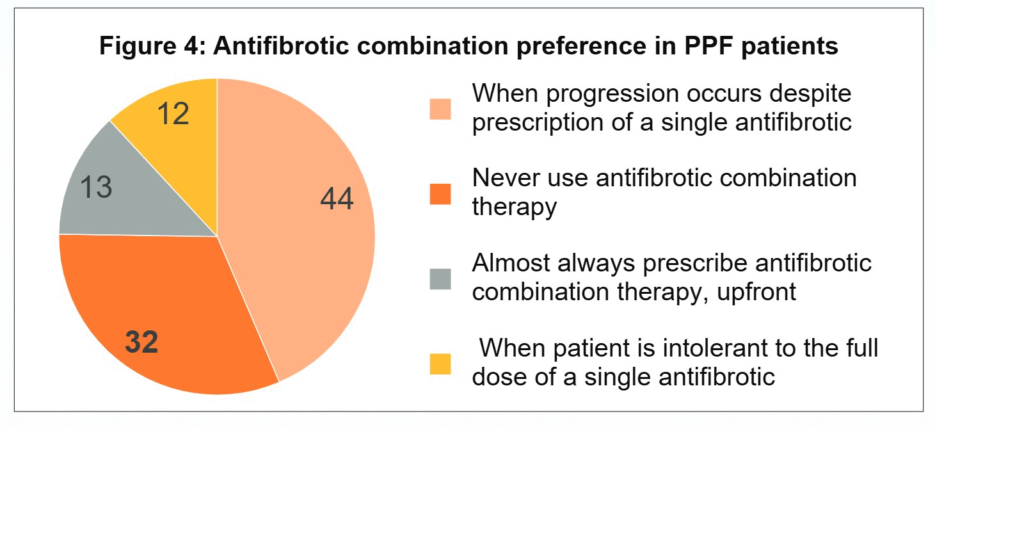
Antifibrotic Use
- 44% clinicians considered antifibrotic combination therapy when progression occurred despite single antifibrotic.
- 13% used combination therapy upfront.
- 12% when single antifibrotic not tolerated (Figure 4).
Pulmonary Rehabilitation & Palliative Care
- 61% offered Pulmonary Rehabilitation (PR) routinely.
- 71% continued PR as long as the patient wished.
- Palliative care initiated in:
- 15% (post-treatment initiation)
- 22% (symptoms worsen despite treatment)
- 27% (NIV-dependent), 26% (O₂-dependent)
Lung Transplant Referral
- Done early if no contraindications (29%).
- 27%, 11%, and 13% referred only in specific scenarios (refractory hypoxemia/NIV dependence).
- 20% did not refer for transplant.
Summary & Conclusions
- Steroid dose escalation is a common first step before antifibrotic initiation.
- Nintedanib – preferred antifibrotic in established PPF.
- Nearly half the clinicians used dual antifibrotic therapy for progression on single antifibrotic.
- PPF management in India shows reliance on clinical judgment, steroids, and gradual antifibrotic introduction.
Thanks
Other Articles

Next
Previous
October 24, 2025
Sabacure Nebpules (Levosalbutamol Sulphate Nebulization Solution)



")